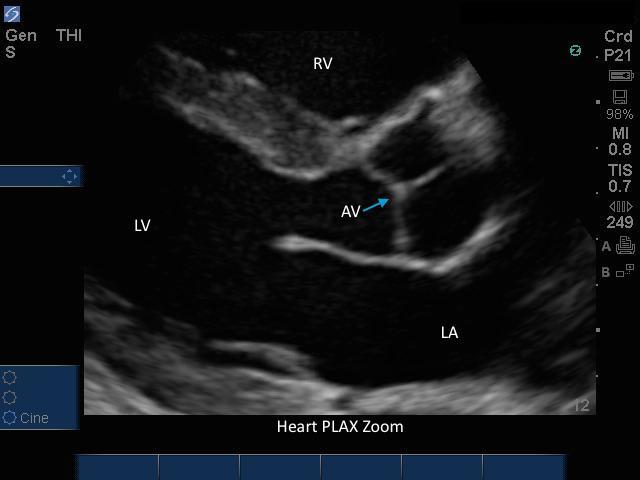
Heart PLAX Zoomed Heart PLAX Zoomed Read more about Heart PLAX Zoomed /sites/default/files/201408_IMAGE_EDGE_HEART_PLAX_ZOOMED.jpg Media Library Type Image Media Library Tag 4 Chamber Aortic Valve Cardiac Cardiac Arrest Cardiac Output Cardiomyopathy Chest Pain Contractility Echo Ejection Fraction Fluid Focused Hypotension Image Left Atrium Left Ventrical Left Ventrical Outflow Track Liver Mitral Valves Parasternal Long Axis Pericardial Pericardial Effusion Pulmonary Emboli Right Ventrical Rt Atrium Septal Soundbyte Cases Tamponde Trauma Volume Window X-Porte
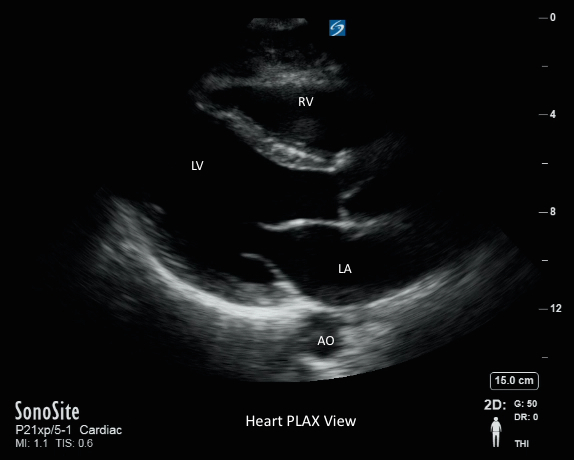
Heart - PLAX View Heart - PLAX View Read more about Heart - PLAX View /sites/default/files/201408_IMAGE_X-PORTE_HEART_PLAX.jpg Media Library Type Image Media Library Tag 4 Chamber Aortic Valve Cardiac Cardiac Arrest Cardiac Output Cardiomyopathy Chest Pain Contractility Echo Ejection Fraction Fluid Focused Hypotension Image Left Atrium Left Ventrical Left Ventrical Outflow Track Liver Mitral Valves Parasternal Long Axis Pericardial Pericardial Effusion Pulmonary Emboli Right Ventrical Rt Atrium Septal Soundbyte Cases Tamponde Trauma Volume Window X-Porte
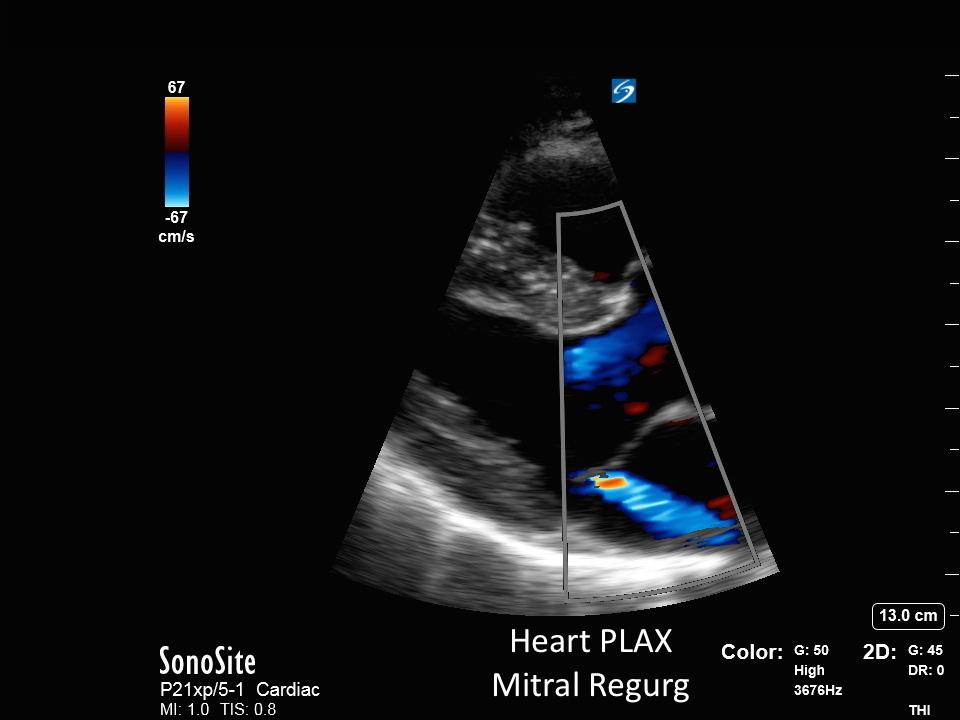
Heart - PLAX Mitral Regurg Heart - PLAX Mitral Regurg Read more about Heart - PLAX Mitral Regurg /sites/default/files/201408_IMAGE_X-PORTE_HEART_PLAX_MITRAL_REGURG.jpg Media Library Type Image Media Library Tag 4 Chamber Aortic Valve Cardiac Cardiac Arrest Cardiac Output Cardiomyopathy Chest Pain Contractility Echo Ejection Fraction Fluid Focused Hypotension Image Left Atrium Left Ventrical Left Ventrical Outflow Track Liver Mitral Valves Parasternal Long Axis Pericardial Pericardial Effusion Pulmonary Emboli Right Ventrical Rt Atrium Septal Soundbyte Cases Tamponde Trauma Volume Window X-Porte