Case: Cardiac Ultrasound - Apical View
Using the apical view and a phased array probe during bedside cardiac ultrasound examinations can enable clinicians to evaluate cardiac health, structures, & ventricular contractility. This view is ideal for identifying cardiomyopathy, pericardial effusion, and cardiac tamponade.
Phil Perera, the emergency ultrasound coordinator at New York Presbyterian Hospital in New York City, introduces "Soundbytes Cases," a series focusing on cardiac ultrasound or echocardiography. This module delves into the apical view of the heart, known as probe position C, following previous examinations of parasternal and subxiphoid views. The apical view is favored by cardiologists for its comprehensive depiction of all four heart chambers and their synergy.
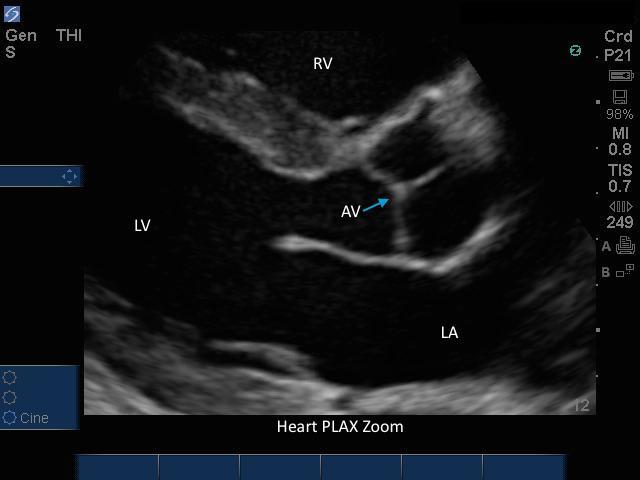
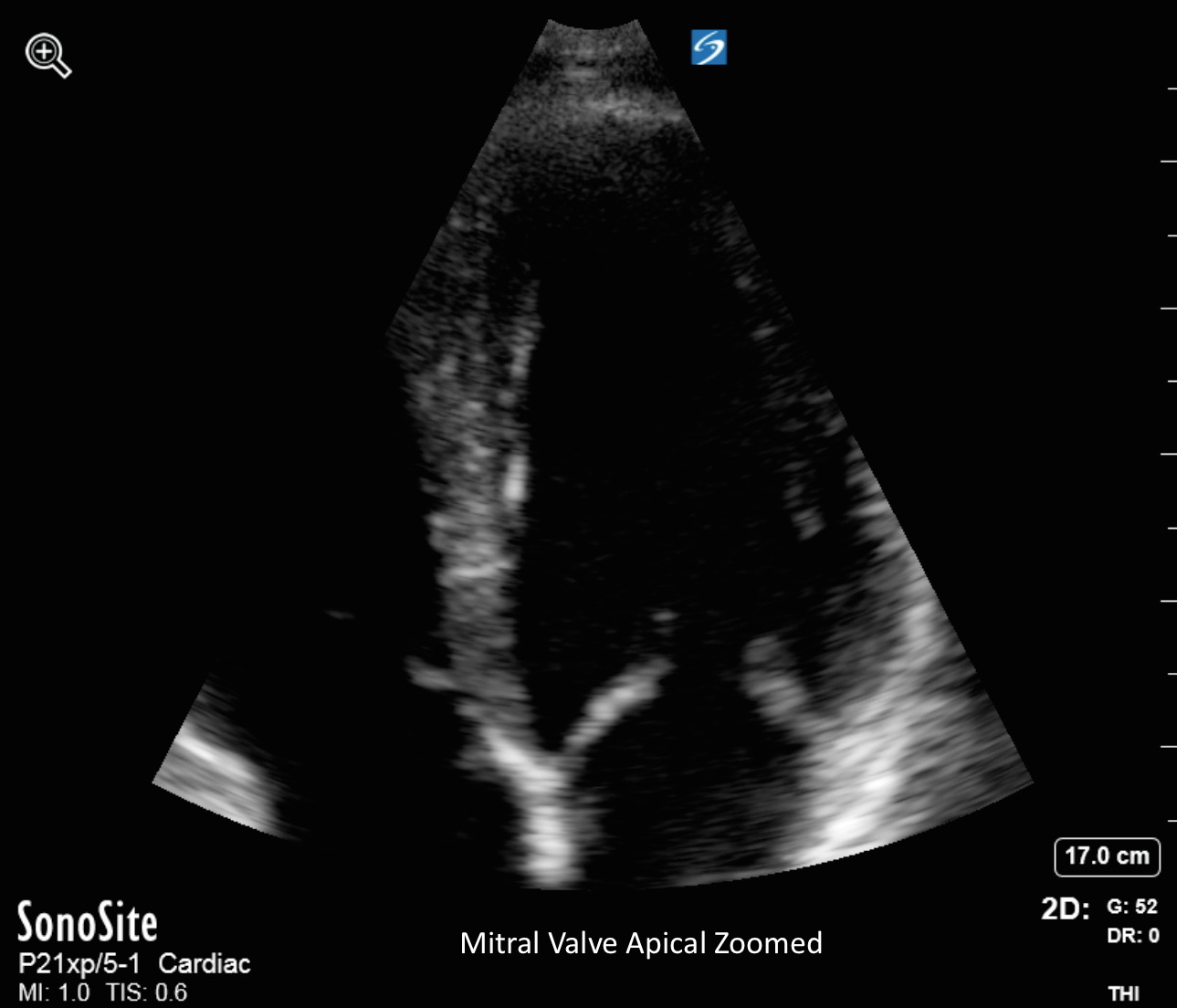
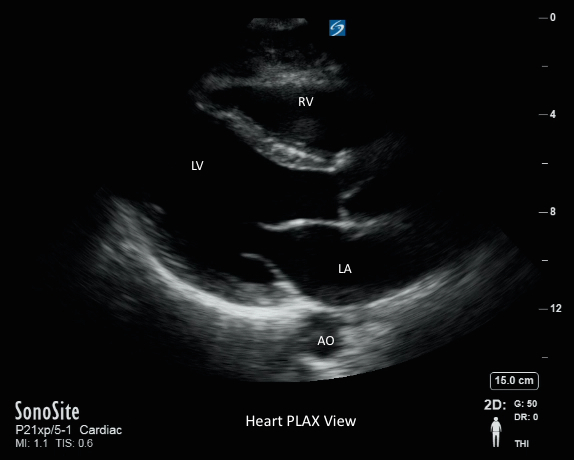
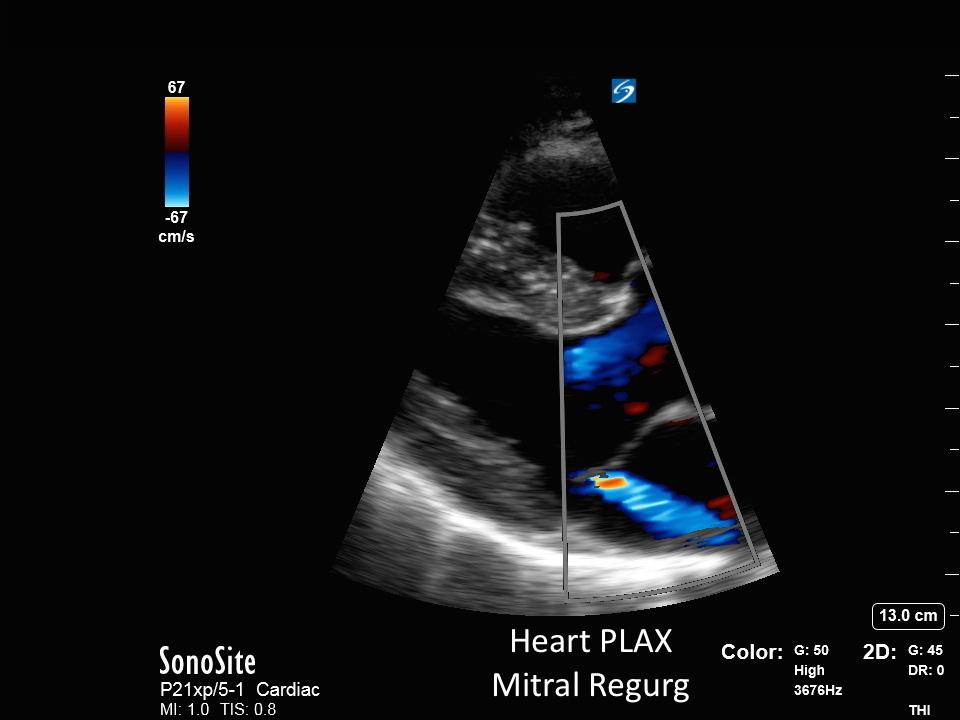
Perera details the technique for obtaining this view, recommending a small phased array probe positioned beneath the left nipple at the point of maximal impulse, with the patient ideally in the left lateral decubitus position for optimal imaging. Interpretation involves identifying ventricles closer to the probe, with atria positioned further away, alongside valves and the pericardium. Video clips illustrate normal and abnormal findings, such as good contractility versus dilated cardiomyopathy and pericardial effusion indicative of cardiac tamponade. Perera underscores the importance of integrating the apical view into cardiac echo examinations routinely.
Perera underscores the importance of integrating the apical view into cardiac echo examinations routinely. Watch the video for details and full context.