

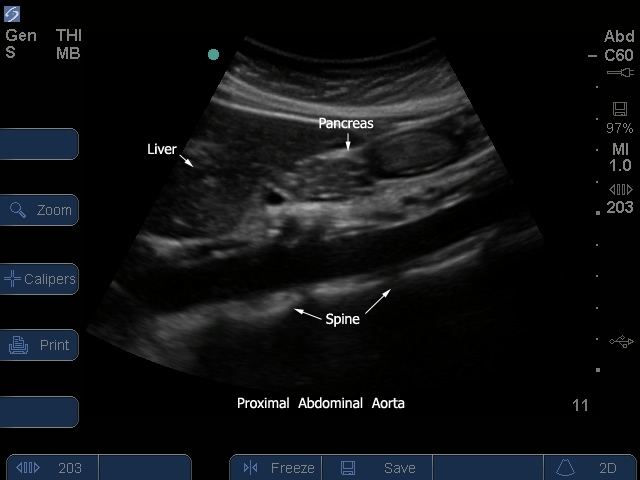
S Series: Proximal Aorta Sagitial View/Diaphraghm
S Series: Proximal Aorta Sagitial View/Diaphraghm

/sites/default/files/201410_Image_S-System_Prox_Aorta_Sagital_1.jpg
S Series: Proximal Aorta Sagitial View/Diaphraghm
Clinical Specialties
Media Library Type
Media Library Tag
Body
S Series: Proximal Aorta Sagitial View/Diaphraghm
S-System: Prox Aorta Sagital 2
S-System: Prox Aorta Sagital 2

/sites/default/files/201410_Image_S-System_Prox_Aorta_Sagital_2_0.jpg
S-System: Proximal Aorta Sagital View 2.
Clinical Specialties
Media Library Type
Media Library Tag
Compatible Products
S-Series: Proximal Aorta Sagital View
S-Series: Proximal Aorta Sagital View
/sites/default/files/201410_Image_S-System_Prox_Aorta_Sagital_2.jpg
S Series: Proximal Aorta Sagital View
Clinical Specialties
Media Library Type
S Series: Proximal Aorta / Celiac - SMA Arteries
S Series: Proximal Aorta / Celiac - SMA Arteries

/sites/default/files/201410_Image_S-System_Prox_Aorta_Celiac_SMA_Arteries.jpg
S Series: Proximal Aorta Celiac SMA Arteries.
Clinical Specialties
Media Library Type
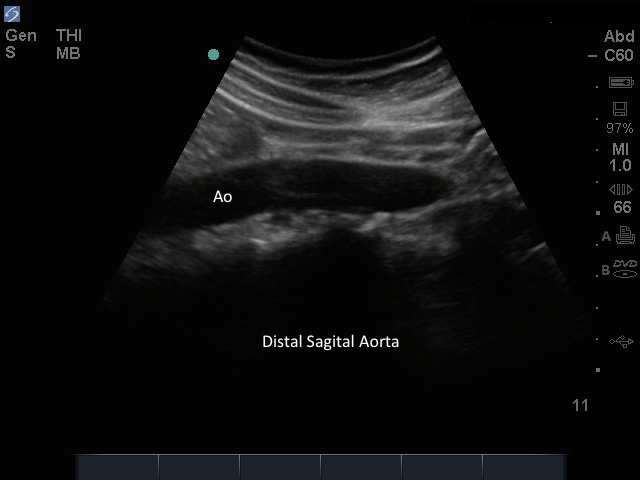
M-Turbo: Distal Aorta Sagital
M-Turbo: Distal Aorta Sagital
/sites/default/files/201410_Image_M-Turbo_Distal_Aorta_Sagital.jpg
M-Turbo: Distal Aorta Longitudinal View.
Clinical Specialties
Media Library Type
Media Library Tag
Compatible Products