Edge: Aorta Sagital Edge: Aorta Sagital Read more about Edge: Aorta Sagital /sites/default/files/201408_IMAGE_EDGE_AORTA_SAGITAL.jpg Media Library Type Image Media Library Tag Abd Abdomen Abdominal Aneurysm Aorta Arterial Blood Disecting Distal Edge False Lumen Focused Free Fluid Fusiform Hemmorrhage Hypotension Iliacs Image Lumen Mid Proximal Rupture Sacular Soundbytes Cases Thrombus Trauma
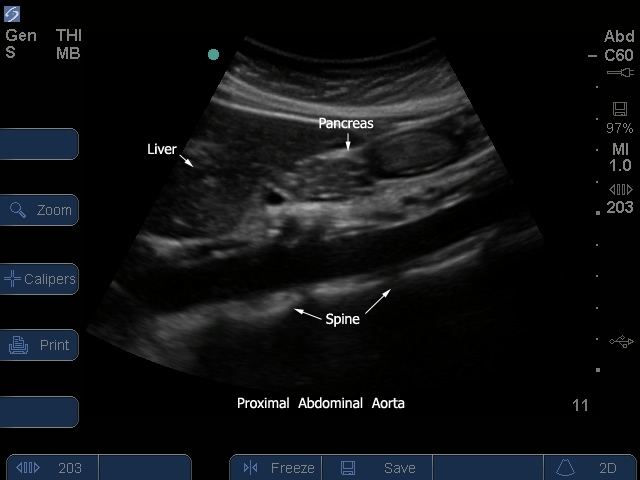
S Series: Proximal Aorta Sagitial View/Diaphraghm S Series: Proximal Aorta Sagitial View/Diaphraghm Read more about S Series: Proximal Aorta Sagitial View/Diaphraghm /sites/default/files/201410_Image_S-System_Prox_Aorta_Sagital_1.jpg S Series: Proximal Aorta Sagitial View/Diaphraghm Clinical Specialties FP/GP Media Library Type Image Media Library Tag S-System Image Aorta Aneurysm Sacular Disecting Fusiform Blood Free Fluid Rupture Lumen Arterial Proximal Mid Distal Iliacs False Lumen Thrombus Focused Trauma Abdominal Abd Abdomen Hypotension Hemmorrhage Body S Series: Proximal Aorta Sagitial View/Diaphraghm
S-System: Prox Aorta Sagital 2 S-System: Prox Aorta Sagital 2 Read more about S-System: Prox Aorta Sagital 2 /sites/default/files/201410_Image_S-System_Prox_Aorta_Sagital_2_0.jpg S-System: Proximal Aorta Sagital View 2. Clinical Specialties FP/GP Media Library Type Image Media Library Tag M-Turbo Aorta Aneurysm Sacular Disecting Fusiform Blood Free Fluid Rupture Lumen Arterial Proximal Mid Distal Iliacs False Lumen Thrombus Focused Trauma Abdominal Abd Abdomen Hypotension Hemmorrhage Compatible Products Sonosite M-Turbo
S-Series: Proximal Aorta Sagital View S-Series: Proximal Aorta Sagital View Read more about S-Series: Proximal Aorta Sagital View /sites/default/files/201410_Image_S-System_Prox_Aorta_Sagital_2.jpg S Series: Proximal Aorta Sagital View Clinical Specialties FP/GP Media Library Type Image Media Library Tag S-System Image Aorta Aneurysm Sacular Disecting Fusiform Blood Free Fluid Rupture Lumen Arterial Proximal Mid Distal Iliacs False Lumen Thrombus Focused Trauma Abdominal Abd Abdomen Hypotension Hemmorrhage
S Series: Proximal Aorta / Celiac - SMA Arteries S Series: Proximal Aorta / Celiac - SMA Arteries Read more about S Series: Proximal Aorta / Celiac - SMA Arteries /sites/default/files/201410_Image_S-System_Prox_Aorta_Celiac_SMA_Arteries.jpg S Series: Proximal Aorta Celiac SMA Arteries. Clinical Specialties FP/GP Media Library Type Image Media Library Tag Aorta Aneurysm Sacular Disecting Fusiform Blood Free Fluid Rupture Lumen Arterial Proximal Mid Distal Iliacs False Lumen Thrombus Focused Trauma Abdominal Abd Abdomen Hypotension Hemmorrhage
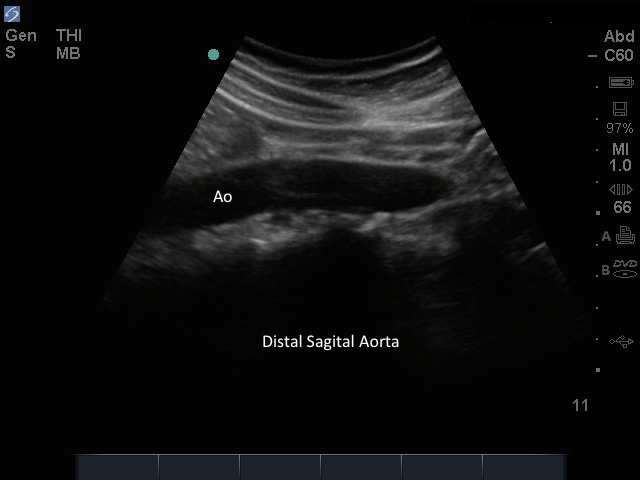
M-Turbo: Distal Aorta Sagital M-Turbo: Distal Aorta Sagital Read more about M-Turbo: Distal Aorta Sagital /sites/default/files/201410_Image_M-Turbo_Distal_Aorta_Sagital.jpg M-Turbo: Distal Aorta Longitudinal View. Clinical Specialties FP/GP Media Library Type Image Media Library Tag Abd Abdomen Abdominal Aneurysm Aorta Arterial Blood Disecting Distal False Lumen Focused Free Fluid Fusiform Hemmorrhage Hypotension Iliacs Lumen M-Turbo Mid Proximal Rupture Sacular Thrombus Trauma Compatible Products Sonosite M-Turbo