GB Stones GB Stones Read more about GB Stones /sites/default/files/201408_IMAGE_EDGE_GB_STONE_ASCITIES.jpg Media Library Type Image Media Library Tag Abd Abdomen Basic Bile Biliary Cholecystitis Cholelithiasis Disease Edge Gallbladder Gallstones Hepatobillary Image Pain Pathology Right Upper Quadrant Soundbytes Cases Stones
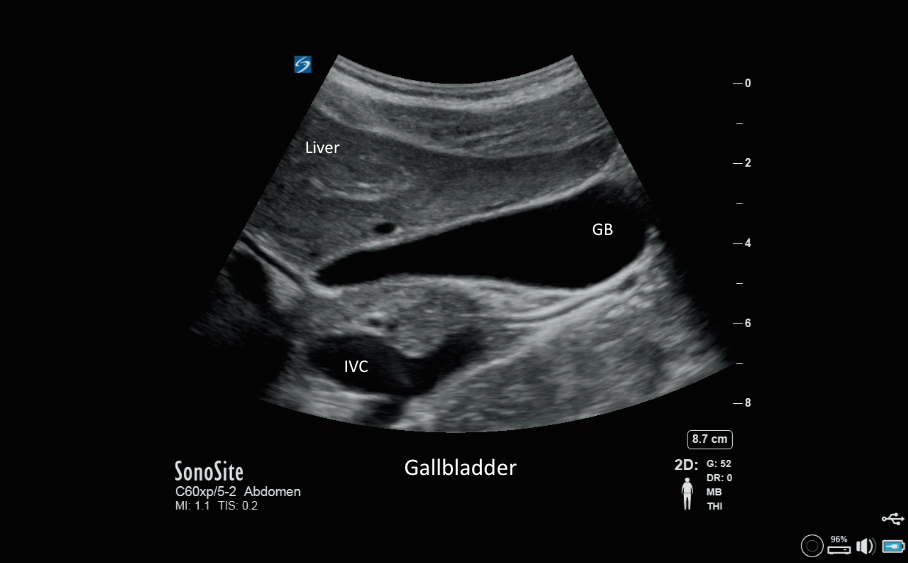
Gallbladder Gallbladder Read more about Gallbladder /sites/default/files/201408_IMAGE_EDGE_GALLBLADDER.jpg Clinical Specialties FP/GP Media Library Type Image Media Library Tag Gallbladder Disease Stones Abdomen Abd Pain Cholecystitis Cholelithiasis Biliary Bile Right Upper Quadrant Basic Pathology Hepatobillary Gallstones Soundbytes Cases Edge Image
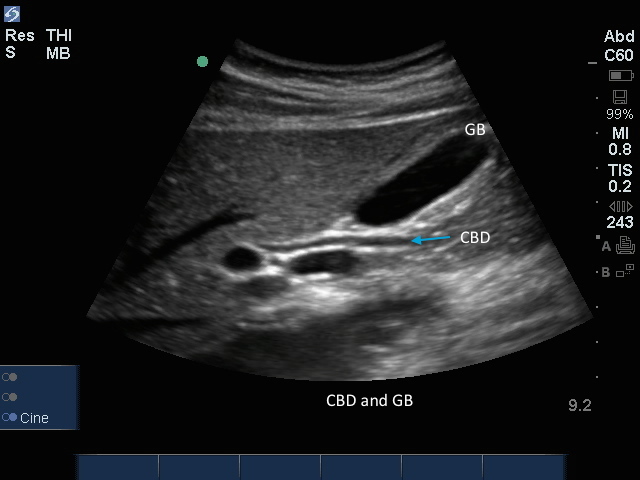
CBD with Gallbladder CBD with Gallbladder Read more about CBD with Gallbladder /sites/default/files/201408_IMAGE_EDGE_CBD_GALLBLADDER.jpg Clinical Specialties FP/GP Media Library Type Image Media Library Tag Gallbladder Disease Stones Abdomen Abd Pain Cholecystitis Cholelithiasis Biliary Bile Right Upper Quadrant Basic Pathology Hepatobillary Gallstones Soundbytes Cases Edge Image Compatible Products Sonosite Edge
Edge: Aorta Sagital Edge: Aorta Sagital Read more about Edge: Aorta Sagital /sites/default/files/201408_IMAGE_EDGE_AORTA_SAGITAL.jpg Media Library Type Image Media Library Tag Abd Abdomen Abdominal Aneurysm Aorta Arterial Blood Disecting Distal Edge False Lumen Focused Free Fluid Fusiform Hemmorrhage Hypotension Iliacs Image Lumen Mid Proximal Rupture Sacular Soundbytes Cases Thrombus Trauma
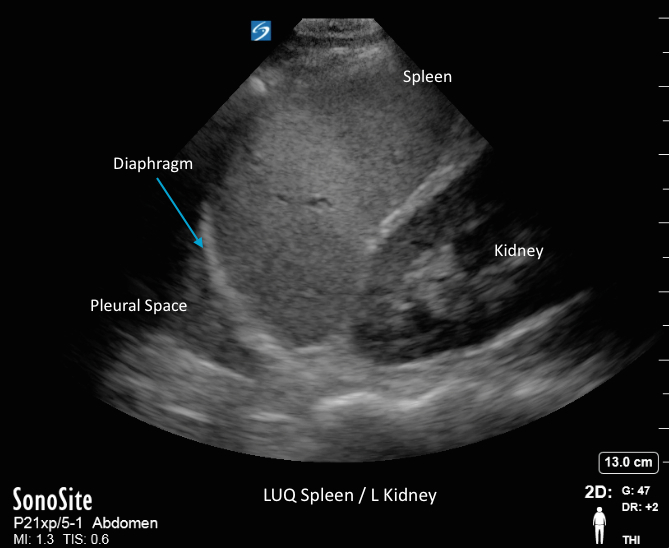
LUQ Spleen/L Kidney LUQ Spleen/L Kidney Read more about LUQ Spleen/L Kidney /sites/default/files/201408_IMAGE_X-PORTE_SPLEEN_LUQ.jpg Media Library Type Image Media Library Tag Abdomen Abdominal Ascities Blood Diaphragm Fluid Fluid Collection Focused Free Fluid Hemorragic Hemorrhage Hypotension Image Kidney Left Upper Quadrant Soundbytes Cases Spleen Trauma Triage X-Porte
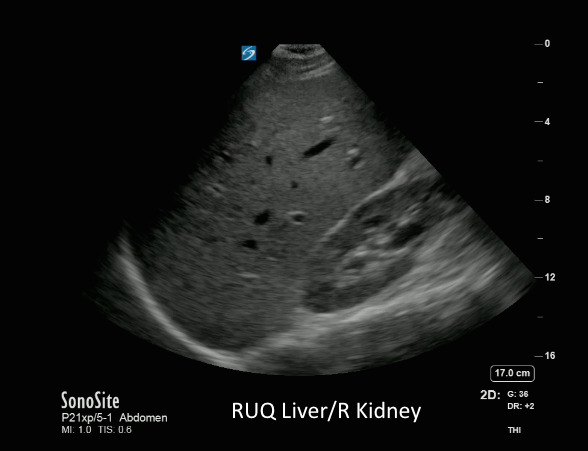
RUQ Liver/R Kidney1 RUQ Liver/R Kidney1 Read more about RUQ Liver/R Kidney1 /sites/default/files/201408_IMAGE_X-PORTE_RUQ_LIVER_R_KIDNEY.jpg Media Library Type Image Media Library Tag Abdomen Abdominal Ascities Blood Collections Diaphragm Fluid Focused Free Fluid Hemorragic Hypotension Image Kidney Liver Morison's Pouch Right Upper Quadrant Trauma Triage X-Porte
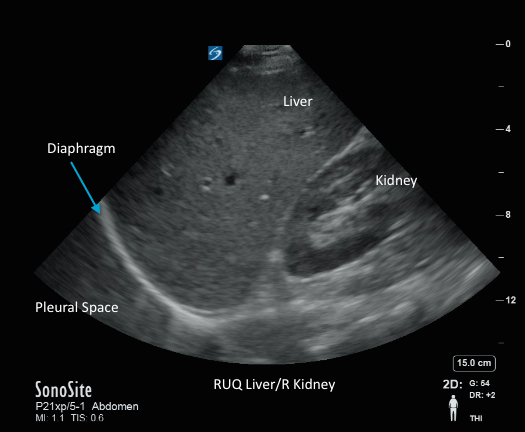
RUQ Liver/R Kidney RUQ Liver/R Kidney Read more about RUQ Liver/R Kidney /sites/default/files/201408_IMAGE_X-PORTE_LIVER_RT_KIDNEY_RUQ.jpg Media Library Type Image Media Library Tag Abdomen Abdominal Ascities Blood Collections Diaphragm Fluid Focused Free Fluid Hemorragic Hypotension Image Kidney Liver Morison's Pouch Right Upper Quadrant Trauma Triage X-Porte
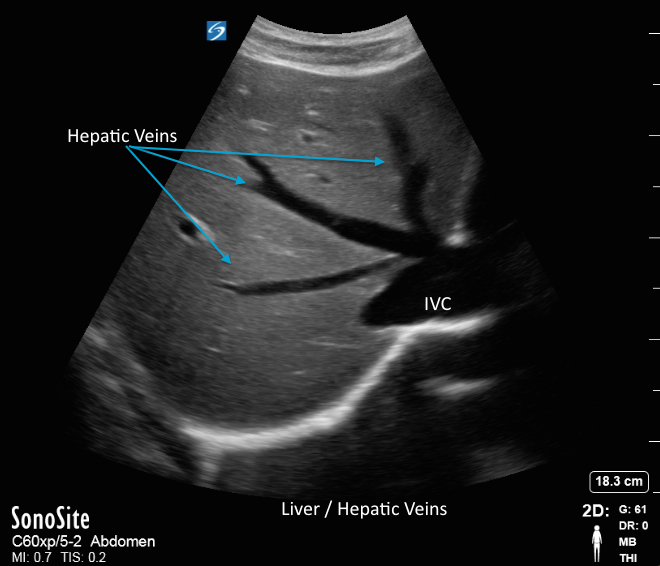
Liver/Hepatic Veins Trv Liver/Hepatic Veins Trv Read more about Liver/Hepatic Veins Trv /sites/default/files/201408_IMAGE_X-PORTE_LIVER_HEPATIC_VEINS.jpg Media Library Type Image Media Library Tag Abdomen Abdominal Ascities Blood Collections Diaphragm Fluid Focused Free Fluid Hemorragic Hypotension Image Kidney Liver Morison's Pouch Right Upper Quadrant Trauma Triage X-Porte Compatible Products Sonosite X-Porte
Gallbladder 09 Gallbladder 09 Read more about Gallbladder 09 /sites/default/files/201408_IMAGE_X-PORTE_GALLBLADDER.jpg Clinical Specialties FP/GP Media Library Type Image Media Library Tag Gallbladder Disease Stones Abdomen Abd Pain Cholecystitis Cholelithiasis Biliary Bile Right Upper Quadrant Basic Pathology Hepatobillary Gallstones Image X-Porte Compatible Products Sonosite X-Porte